The International Medication Safety Network (IMSN) is an international network of established safe medication practice centres, operating medication error reporting programmes and producing guidance to minimise preventable harms from medicine use in practice. IMSN promotes safer medication practice to improve patient safety internationally. About IMSN
The International Medication Safety Network (IMSN) mourns the death of David Cousins, on May 22, 2023 in his home with his family by his side. This is what his wife Trina told us the next day “The sun was shining in through the windows as he gently took his last breath. It was a beautiful moment”, asking us to “remember him as a great, friend, colleague, musician, biker and above all a wonderful husband and father”.
Like most of the IMSN's founders, David Cousins was a busy hospital pharmacist. As chief pharmacist of Derby Hospitals (September 1983–August 2002), he commissioned a new pharmacy department and provided a range of new pharmacy services: - full intravenous additive service; pump and syringe driver library service; - aseptic satellite pharmacies in intensive care, paediatrics, cancer care, operating theatres and, palliative care/hospice; - pharmacists as full members of the cardiopulmonary resuscitation team. He developed a substantial commercial aseptic dispensing business as income generation for the hospital, selling total parenteral nutrition, antibiotics, chemotherapy and other intravenous infusions to home care companies and hospitals. He also introduced new postgraduate pharmacy training courses in the UK with the University of Derby: DPharm, MSc and Postgraduate diploma for pharmacists and validated training courses for pharmacy technicians.
David Cousins was also Fellow of the Royal Pharmaceutical Society (RPS) and active member of the UK Clinical Pharmacy Association (UKCPA) and of the European Association of Hospital Pharmacists (EAHP).
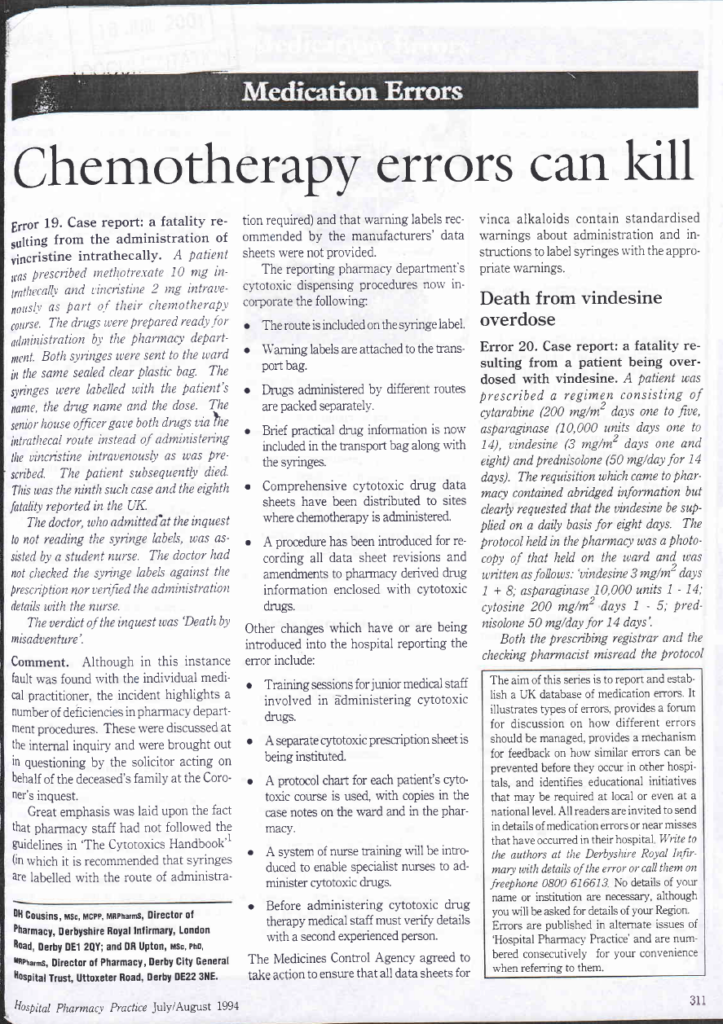
Since 1990, David Cousins developed his research and publications on medication error prevention. Together with David Upton, he wrote a monthly column on medication errors in the journal Hospital Pharmacy Practice, further Pharmacy in practice, whose archives are unfortunately not available in digital format.
His colleagues abroad knew David Cousins mainly as Head of Safe Medication Practice and Medical Devices, National Patient Safety Agency (NPSA) and further NHS England (September 2002 – October 2014), where he helped to develop and implement the NHS National Reporting and Learning System (NRLS). This tireless analyst of tens of thousands of incident reports, NHS complaints and evidence data has published over 50 Patient Safety Alerts and other national guidance intended to minimize preventable deaths and serious harm to patients from the unsafe use of medicines and medical devices including guidance on: the safer use of concentrated potassium chloride Injection; reducing harms from injectable medicines; minimizing wrong route errors including oral liquid medicines, intrathecal vincristine, intravenous bupivacaine; reducing harm from omitted and delayed medicines. So many treasures now only accessible in NHS archives.
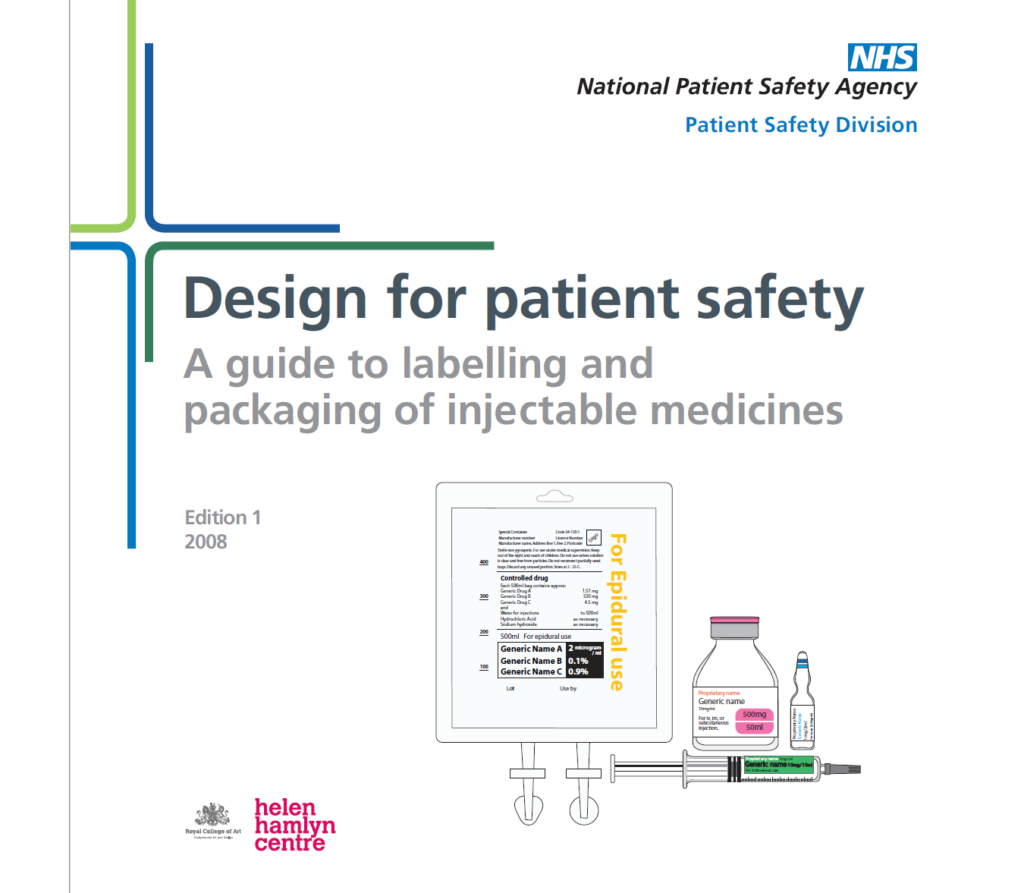
David Cousins inspired and provided technical support to the “Design for Safety” publication series, illustrating how good design can help minimize risk to patients arising from labeling and packaging of medicines. Today, everyone still refers to the reference series on “Design for safety” guidance on labelling and packaging of medicines and design of infusion devices, awarded as the ‘best management of design in a public or non-profit organisation’ category at the Design Management Europe Awards 2008.
At the end of 2007, in collaboration with the National Institute for Health and Clinical Excellence (NICE), he introduced in the UK medicines reconciliation on hospital admission to ensure that any medication patients are taking prior to admission to hospital is properly documented on admission. He also authored a 2014 Patient Safety Alert requiring every NHS organization in England to appoint a Medication Safety Officer. His most enduring legacy is the national network of Medication Safety Officers he launched.
During this period of national responsibility, and on behalf of the UK NPSA, David Cousins was also particularly active at European and international level. As member of the Expert Group on Safe Medication Practices established in 2003 by the Council of Europe Committee of Experts on Pharmaceutical Questions, he played a decisive role in including a specific strategy to promote medication safety in the Council of Europe Recommendation Rec(2006)7 of the Committee of Ministers to member states on management of patient safety and prevention of adverse events in health care adopted 24 May 2006. It is regrettable that the report approved on November 7, 2006, to which he contributed and that he presented on many occasions, is no longer available on the European Directorate for the Quality of Medicines & HealthCare (EDQM) website.
Airaksinen, M., Otero, M-J., Schmitt, E., Cousins, D., Gustafsen, I., Hartmann, M., Lyftingsmo, S., Muff, P., Thors, C-E., Vlcek, J., & Expert Group on Safe Medication Practices “Creation of a better medication safety culture in Europe: building up safe medication practices” Council of Europe 2006; 278 pages. Read on…
After lobbying the Council of Europe to set up a European network of national safe medication practice centres “with the aim of sharing information concerning risks, including medicine products and practices, reporting methods, analysis and promoting solutions”, David Cousins took part in the founding of the IMSN and in writing the “Salamanca Declaration To Promote Safe Medication Practices Globally”.
Still on a global scale, David Cousins has been one of the driving forces behind a WHO project under the Seventh Framework Programme of the European Union (EU-FP7), aiming to increase the capacity of pharmacovigilance (PV) centres in identifying and understanding the root causes of preventable adverse drug reactions (ADRs) (2009 - 2013).
After an unforgettable workshop held in 2011 in the Morocco Poison and Pharmacovigilance Centre, partnering with the WHO and the Uppsala Monitoring Centre (Sweden), he contributed to a seminal report “Reporting and learning systems for medication errors: the role of pharmacovigilance centres” published in 2014.
David Cousins also tried to orient the European Medicine Agency’s (EMA) policy on preventing medication errors.
After the dismantling of the NPSA to which he had devoted so much time and effort, David Cousins became Head of Patient Safety, Healthcare at Home (October 2014 – March 2018), where he built a new complaints and patient incident reporting system, implemented in March 2016. During this period he worked with the NHS and other stakeholders to develop new standards on managing complaints and incidents within homecare services. During his retirement David Cousins has been advising for the patient charity, Action against Medical Accidents (AvMA), publishing in particular "An organisation losing its memory" in January 2020.
David Cousins was convinced, determined and pugnacious, as shown by his positions in reaction to what he saw as resignations. He became recipient of the RPS Lifetime Achievement Award, the 2015 UKCPA Lifetime Achievement Award and the 2020 ISMP Lifetime Achievement Cheers Award, pleased to receive recognition from peers.
In his response during the ISMP Cheers Awards ceremony, David Cousins said: “I describe how I first got interested in medication errors and their prevention, first publishing medication error incidents in a pharmacy journal, and my work at the National Patient Safety Agency and other organisations. We made significant progress in England between 2002 – 2014, however in recent years this progress has not been maintained. The work of ISMP, IMSN and other organisations continues to be vital to continue to improve knowledge of medication errors and their prevention. I wish you all every success in the future.”
Mike Cohen, Chair of the IMSN told : "David is known world-wide for his important work in medication safety over many years. He was one of the organizers of the International Medication Safety Network and will be remembered for his life-saving work and the many contributions he made to the work we all share." June 2023
Intravenous (IV) oxytocin is used antepartum to induce labor in patients with a medical indication, to stimulate or reinforce labor in selected cases of uterine inertia, and as an adjunct in the management of an incomplete, inevitable, or elective abortion. Used postpartum, IV oxytocin is indicated to produce uterine contractions during the expulsion of the placenta, and to prevent or control postpartum bleeding or hemorrhage. Therefore, oxytocin is needed in all obstetric care areas with consistency of practice amongst all provider types (e.g., anesthesia, obstetrics, midwives, perinatal nursing) whether using low doses for labor induction or augmentation, commonly measured in milliunits, or at higher doses to prevent or treat postpartum hemorrhage (PPH), commonly measured in units.
However, improper administration of oxytocin can cause hyperstimulation of the uterus, which in turn can result in fetal distress, the need for an emergency cesarean section, or uterine rupture. Multiple International Medication Safety Network (IMSN) member countries have identified that there are substantial risks involved with the use of oxytocin and have reported significant patient harm from related errors
As a result, the executive committee formed the IMSN Oxytocin Safety Interest Group (OxytocinSIG) to further address the safe use of oxytocin globally. The two primary objectives of the initiative were to share issues and errors on use and administration of oxytocin among members and to develop comprehensive and global applicable recommendations including a guidance document on safe use of oxytocin.
Building a Response to Oxytocin-Related Errors
In a series of OxytocinSIG meetings held in 2022, IMSN members shared firsthand experience with a variety of risks, close calls, errors, and adverse events associated with the use of oxytocin. These included:
Inappropriate/unnecessary use in labor induction in low-risk patient populations
Lack of a standardized dosing regimen
Confusion with look-alike and sound-alike medications
Inappropriate use of brand names or unsafe abbreviations
Non-standardized or non-centralized preparation of oxytocin infusions
Use of multiple oxytocin infusion concentrations/preparations
Insuficient monitoring of beyond-use dates of pre-prepared solutions
Reliance on manually programmed infusion pumps without automated safeguards in place
Mix-ups with infusion tubing
Mix-ups with dosing/infusion rates
Use/availability of oxytocin in the direct patient care area without appropriate orders and communication among healthcare providers
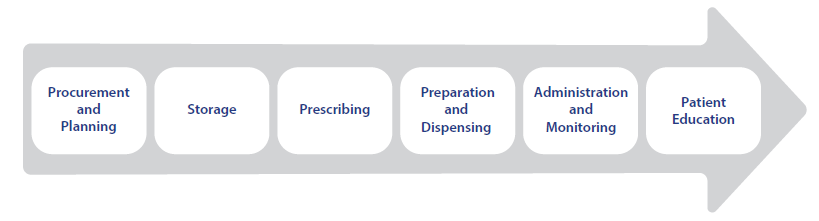
IMSN Oxytocin SIG Recommendations for Global Implementation of Safe Oxytocin Use Practices
These selected risk-reduction strategies include recommendations that can help avoid errors and significant patient harm related to the use of oxytocin through all phases of the medication-use process.
The risk-reduction strategies include high-leverage forcing functions and computerization in addition to less technologically based recommendations. These key improvements must be accompanied by low-leverage strategies, such as staff education, patient education and counseling, and warnings and reminders. Combining low-, moderate-, and high-leverage strategies work to exponentially enhance safe oxytocin utilization.
For a complete copy of the IMSN Oxytocin SIG Recommendations for Global Implementation of Safe Oxytocin Use Practices, click here.
Implementing and moving forward
IMSN acknowledges that healthcare organizations in different parts of the world vary in the availability of technologies (e.g., electronic health records, infusion pumps, automated dispensing cabinets) and resources (e.g., central pharmacy compounding programs). While the recommendations may not all be achievable everywhere, organizations should work to identify those that can be implemented at each step of the medication-use process and consider the remaining recommendations as future goals to work towards.
Continue to report errors involving oxytocin through your normal reporting programs and to the International Medication Error Reporting Portal, so that we may continue to evaluate the safe use of oxytocin and other medications around the world.
Premixed solutions are currently not available globally except from outsourced compounding pharmacies in some countries. IMSN urges the global pharmaceutical industry to make premixed oxytocin solutions available everywhere, as soon as possible.
During the fall of 2020, as the world waited in anticipation for the emergency use/conditional marketing authorization of COVID-19 vaccines, members of the International Medication Safety Network (IMSN) began to discuss safety issues that might impact global immunization roll out efforts with regard to the knowledge on vaccination errors already gathered by the IMSN.
With the goal of sharing experience and learning from member countries to address COVID-19 vaccine safety issues, the IMSN Executive Committee formed the IMSN COVID-19 Vaccine Safety Interest Group (CVSIG) in February 2021. The two primary objectives of the initiative were to address issues encountered by members during global vaccine rollout and to create a guiding document of experience-based safety recommendations.
Building a Response to the Different Types of Vaccine-Related Errors
In a series of CVSIG meetings in mid-2021, as vaccination campaigns rolled out, IMSN members shared firsthand experience with a variety of risks, near-misses, errors, and adverse events following immunization with COVID-19 vaccines on the basis of aggregated analysis by CVSIG members. These included issues with:
screening (e.g., wrong age, patients with contraindicated conditions),
storage (e.g., inappropriate storage temperature, confusion and mis-selection resulting from storage near other vaccines or monoclonal antibodies),
preparation (e.g., serial errors for vaccines needing a two-step reconstitution process, diluent errors including incorrect diluent volume or no dilution, dosing errors including wrong dose, no dose, expired dose),
administration (e.g., shoulder injury related to vaccine administration, wrong time interval for second dose or third dose, syringe and/or needle malfunction or misuse leading to underdose, wrong vaccine, wrong drug, wrong route of administration, accidental exposure),
and monitoring (e.g., missed second or third doses).
In addition, the approach to errors has evolved over the course of COVID-19 vaccination campaigns (for example, intervals between doses, authorized ages, authorized doses, and recommended vaccines).
IMSN CVSIG Recommendations for Global Implementation of Safe COVID-19 Immunization Practices - January 2022
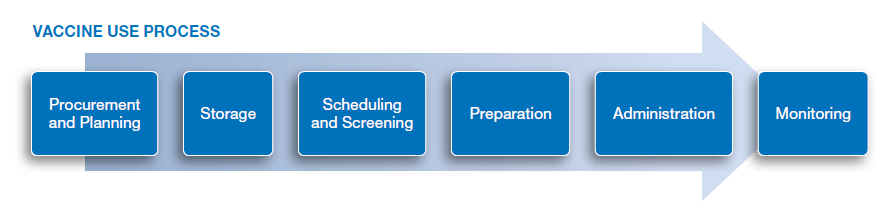
The recommendations follow the vaccine use process and address errors occurring during each stage.
These safety recommendations were developed based on the collective experience and learning from IMSN member countries and should be considered for implementation in global COVID-19 immunization efforts. For a complete copy of the IMSN CVSIG Recommendations for Global Implementation of Safe COVID-19 Immunization Practices, click here.
Moving Forward: during the development of these recommendations, several topics were identified that will receive special attention from IMSN
Promoting packaging vaccines in prefilled unit-dose syringes as a global standard
Addressing issues related to COVID-19 vaccine safety for pediatrics as COVID-19 vaccines are being authorized for use in more countries
Addressing risks during overlapping COVID-19 immunizations and other immunization campaigns
Involving IMSN in review of a globally standardized schema and pathways for adverse events following immunization reporting